
Samantha Newman, National Center for Health Research
The focus of this article is medical transitioning from male to female, the process by which transgender individuals change the way they look so that their physical characteristics match the gender they feel. [2] Transgender is defined as individuals whose social or psychological gender identity is different than their sex assigned at birth. [2]
Transitioning isn’t necessarily medical. It can involve changing one’s name or one’s pronouns. It can involve changing the way one dresses. Medical transitioning can involve medical treatments (hormones) and can involve surgery. Experts agree that there is not one “right” way to transition. Transitioning can involve any combination of these changes or it can be any change that allows someone to more comfortably present to the world. [2] What is most important is that someone’s transition process reflects their needs and what works best for them and their body. [1] While there are many social ways to transition, such as coming out to friends, using different pronouns, or using a different name, this article will specifically examine the medical treatment options in the male to female transition process.
For someone considering medical transitioning, it is important to know the risks that are associated with specific medical treatments and to decide if the likely benefits outweigh those risks. It is essential to realize that many aspects of this medical transition can be very expensive, so make sure to find out what will or will not be covered by insurance. The goal of this article is to provide information to help individuals make an informed choice, choosing the safest options that will provide the most benefit.
Before beginning transgender transitional medical treatment, the World Professional Association for Transgender Health (WPATH) recommends meeting with a mental health professional for a gender dysphoria diagnosis and psychotherapy. [1] According to the American Psychiatric Association, a gender dysphoria diagnosis is when a person’s physical or assigned gender does not match the gender they feel. [23] Most doctors will not offer most medical transitioning options unless the individual has this diagnosis. However, some medical procedures, such as facial feminization surgery or laser hair removal, do not require meeting with a mental health professional beforehand.
After receiving a gender dysphoria diagnosis, one can consider whether or not to choose hormone therapy. If a person chooses hormone therapy, it is usually followed by a period of living publicly as a trans man or woman before major surgeries are performed (this is called the Real-Life Test and it will be discussed later in the article). [3] Hormone therapy is usually recommended prior to most types of surgery. [1]
Each medical intervention has its own unique recommendations and risks.
For trans women, medical transitioning may include any of the following [2]:
· hormone therapy (to create feminine characteristics, such as less body hair, softer skin, and breast growth)
· laser hair removal (to remove hair from face and body)
· tracheal shave (to make the Adam’s apple smaller)
· facial feminization surgery (to create feminine facial features)
· breast augmentation (breast implants)
· orchiectomy (to remove the testes)
· penile inversion vaginoplasty (to create a vagina by inverting penile skin)
Hormone Therapy
There are many types of hormones in our bodies, but estrogen, testosterone, and progestogen are considered sex hormones because they affect sexual characteristics. All males and females have both male and female hormones, but the relative amounts of these hormones in the body give us our specific physical characteristics. [20] For male to female hormone therapy, there are patches, pills, and injections containing estrogen and/or anti-androgens that can help change the arrangement of muscles, skin, and fat distribution, to make the individual appear more feminine. [1]
According to WPATH, the criteria for hormone therapy are as follows:
1. Persistent, well-documented gender dysphoria diagnosis from a mental health professional;
2. Capacity to make a fully informed decision and to consent for treatment;
3. Age of majority (which varies in different countries and states). If a person wanting to transition is younger, there are different rules that can be found in Section VI of the WPATH’s Standard of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People);
4. If an individual who wants to transition already has significant medical or mental health issues, those mental health issues must be reasonably well controlled. [1]
Estrogen and anti-androgens help block some of the masculinizing effects of testosterone, including facial and body hair and male pattern baldness.[4] [1] As a result, the physical effects of hormone therapy also include “breast growth, decreased erectile function, decreased testicular size,” and an increase in the percentage of body fat compared to muscle mass. [1] Most physical changes occur gradually over the course of two years. The amount of physical change and the exact timeline of those changes vary. For more details, see Table 1, which outlines the effects and expected time these effects will take place once hormones are taken as presented in WPATH’s Standard of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People. [1]
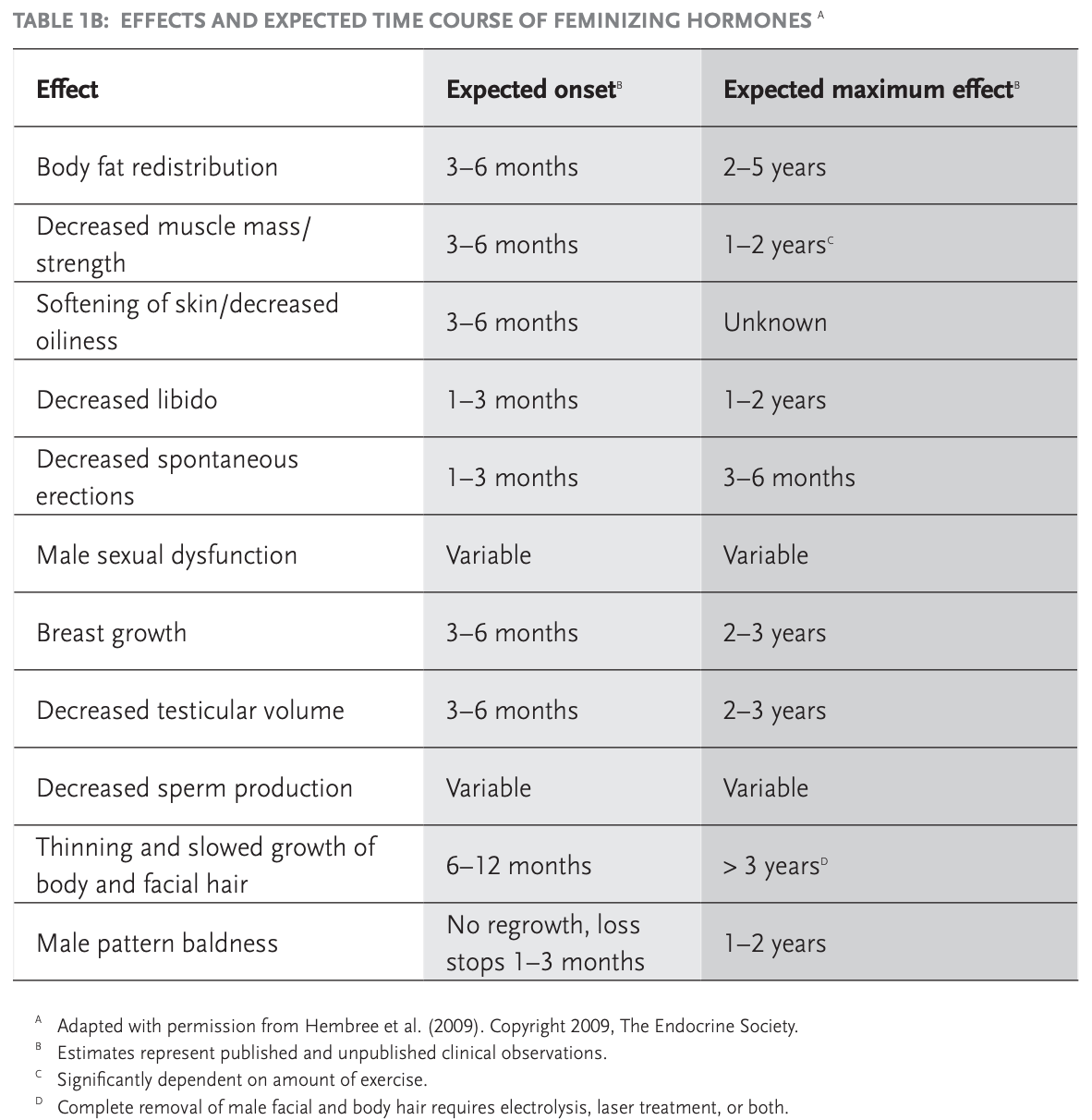
Table 1 taken from WPATH’s Standard of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People
Risks of Hormone Therapy
All medical interventions have risks. According to WPATH, feminizing hormones have an increased risk of a blood clot in a deep vein, usually in the leg, that is called venous thromboembolic disease (VTD) and can be fatal. Other risks include gallstones, elevated liver enzymes, weight gain, cardiovascular disease, and a high level of a certain type of fat (triglycerides) in the blood). [1] There is a possible increased risk of high blood pressure, higher levels of the hormone prolactin, and Type 2 diabetes. It has not been proven whether or not it increases the risk of breast cancer. [1]
Estrogen taken in pill form has more VTD risks than estrogen administered with a transdermal patch on the skin) estrogen administration. Ethinyl estradiol is the type of oral estrogen with a well-documented higher risk for VTD. For that reason, this specific type of oral estrogen should be avoided for feminizing hormone therapy. [1]
Using progestins in feminizing hormone therapy is controversial. Some experts believe it is necessary for full breast development, while others report that progestin hormones do not enhance breast growth. In addition, progestins may increase the risk of breast cancer and cardiovascular disease, and also have risks such as depression and weight gain.[1,5]
As noted above, the effects of hormone therapy are seen gradually over a period of about two years. It is important to understand that taking higher than prescribed doses of hormones DOES NOT increase the speed of the transition process. It can, however, cause dangerous side effects. [20]
Most importantly, never take hormones from oversea mail-order companies, street sellers, or friends. Always go to a licensed physician because they will be able to administer the best dosage of these hormones as well as properly monitor their effects. [20]
Laser Hair Removal and Electrolysis
Laser hair removaldark hairs
LHR is FDA-approved for permanent hair reduction. Patients must be evaluated by a medical provider prior to being treated. [12] Electrolysis uses electric currents from a fine needle shaped probe to destroy the root of individual hair follicles. Electrolysis is FDA-approved for permanent hair removal, and can be used on all hair and skin types. [12] This procedure is effective for targeting hairs that do not respond to LHR. Neither procedure is covered by health insurance.
When choosing between LHR and electrolysis, it depends what a person wants from the procedure. LHR may be done just about anywhere on the face and body, except around the eyes. There is little-to-no recovery time involved. While new hair may still grow, they generally grow finer and lighter in color than before. As a whole, this procedure tends to work best with fair skin and dark hair. [25] Electrolysis is also versatile and produces more permanent results. It can help prevent new hair growth for all skin and hair types. Electrolysis may also be used anywhere on the body, including the eyebrows. However, there are usually more sessions of electrolysis than LHR, which may result in a higher cost for electrolysis procedures. [25]
When choosing a hair removal option, one may also choose to use both types of hair removal processes for different areas of the body. It is important to consult with a physician about skin sensitivities.
Risks of Laser Hair Removal and Electrolysis
Overheating from the lasers can result in redness, blisters, burns, scab formation, and changes in skin color. The procedure itself is also painful and may require the use of topical anesthetics. [12]
Electrolysis has many of the same risks as LHR, including pain, swelling, tiny blisters, scabs, dryness, and ingrown hairs. To reduce the chances of bad side effects, it’s important to choose an experienced and licensed practitioner. [14]
It is also important to note that NEITHER home laser NOR home electrolysis devices have demonstrated effectiveness. Both home devices may actually cause harm. [13]
Tracheal Shave
Tracheal shaveAdam
Risk of a Tracheal Shave
Mild discomfort is expected in the days after this procedure. Other side effects may last a few days and could include bruising, swelling, lumpiness around the neck area, sore throat, mild voice weakness, and some tightness around the neck area. [17]
The incision area may be red and thick for the first few weeks. This is a delicate area and the voice can be affected if too much cartilage is removed. [17] A tracheal shave should only be performed by an experienced and qualified surgeon.
Facial Feminization Surgery
Facial Feminization Surgeries are surgeries meant to create feminine facial features. They usually include or are a combination of procedures such as botox, lip augmentation, chin contouring, chin width reduction (genioplasty) face-lift, eye and lid modification, jaw contouring, forehead contouring, molar/cheek contouring, and nose reshaping (rhinoplasty). [15] Like all surgeries, there are risks. As a patient, it is important to assess personal needs and the risks of the procedure. To read about more various procedure options, visit the Mayo Clinic’s Facial Feminization Surgery page. [19]
According to WPATH, letters of readiness from mental health providers are not necessary for facial feminization surgery. However, mental health professionals can play an integral role in helping one make fully informed decisions about the timing and role of these procedures in the transition process. [1]
However, facial feminization surgery isn’t the best option for every transgender woman. A doctor might recommend against these surgeries if the patient has:
-
Unmanaged mental health conditions
-
Significant health conditions, such as heart or kidney disease, a bleeding disorder, or a history of blood clots in a deep vein (deep vein thrombosis) or in a lung (venous thromboembolism)
-
Any condition that limits the ability to give informed consent [19]
Facial Feminization Surgery Risks
As previously noted, any surgery has risks. The decision to have facial feminization surgery is extremely personal and one must decide if the benefits are worth the risks and potential complications of the surgery. The risks of facial feminization surgeries include (but are not limited to), infection, bleeding, poor healing of incisions, failure of the bone to heal, hematoma (localized bleeding outside of blood vessels), prolonged swelling, implant migraine (where an implanted structure moves away from its original location), hair loss, as well as surgical risks involving anesthesia. [18]
Other short-term complications might include:
· Suture rupture along an incision line
· Fluid accumulation beneath the skin (seroma)
Long-term complications might include:
· Visible scarring
· Dissatisfaction with appearance after surgery
· A facial nerve injury [19]
Breast Augmentation (Breast Implants)
According to WPATH, the criteria for breast augmentation in male to female patients are the same as those for hormone therapy (see above).
In order to achieve the best aesthetic results, it is recommended that male to female transitioning patients undergo feminizing hormone therapy for at least 12 months prior to breast augmentation surgery. [1] Although prior hormone therapy is not always required, think carefully before speeding up the process, and discuss options with a qualified surgeon.
Breast implants can either be filled with saline (salt water) or silicone gel. All breast implants have an outer envelope made of silicone. This envelope can be “smooth” or “textured.” All breast implants have risks, but some types of implants have more risks than others. [6] In general, saline implants with a smooth texture are less dangerous, but may not provide the best aesthetic results. Read here to learn about the different types of breast implants and the risks and benefits of each type of implant. [9]
Risks of Breast Implants
Breast implants have many risks, including rupture, capsular contracture (hardening of scar tissue around the implant which causes pain and hardness), autoimmune symptoms, breast pain or swelling, and infection. The following Patient Informed Consent Checklist includes most of the risks of breast implants: http://breastimplantinfo.org/the-breast-implant-working-groups-breast-implant-black-box-warning-and-patient-checklist/. For more detailed information about the risks and complications of breast implants, see the website of The Breast Implant Information Project. [7] The Breast Implant Information Project also has helpful information about other breast implant alternatives and advice, such as . [8]
Although breast implants have numerous risks, silicone injections are much more dangerous. As stated by the Food and Drug Administration (FDA), silicone from injections can travel to other parts of the body and block blood vessels in the lungs, heart, or brain. This can result in permanent damage to those tissues and lead to stroke or death. [10]
Removal of Testicles
An orchiectomy is a surgical procedure that removes the testicles, since they produce sperm and testosterone. There are several types of orchiectomy procedures and transgender patients are not the only ones undergoing these procedures. For example, a cancer patient may need a different type of orchiectomy procedure than a transgender patient. For transgender patients, either a radical inguinal orchiectomy or a bilateral orchiectomy is recommended. In a radical inguinal orchiectomy, the testicles are removed through a small cut in the lower part of your abdominal area instead of your scrotum. In a bilateral orchiectomy, both testicles are removed from the scrotum. Bilateral orchietomy is more common for male to female transgender patients, but both have shown to be effective surgeries. [11
Male to female patients can also consider sperm preservation options and should be encouraged to consider banking their sperm before hormone therapy. [1]
According to WPATH, “Two referrals—from qualified mental health professionals who have independently assessed the patient—are needed for genital surgery (i.e., hysterectomy/salpingo-oophorectomy, orchiectomy, genital reconstructive surgeries).” One of the referrals can be from the patient’s psychotherapist. [1]
According to WPATH, the criteria for removal of the testes in male to female patients include the same four criteria as those for hormone therapy and breast implants, but also include a fifth criteria:
· 12 continuous months of hormone therapy as appropriate to the patient’s gender goals. (The aim of hormone therapy prior to genital surgery is primarily to introduce a period of reversible estrogen or testosterone suppression, before the patient undergoes an irreversible surgical procedure.) [1]
The surgeon will remove the testicles from the scrotum. During a scrotectomy, the surgeon will remove the entire scrotum or a portion of it. If the patient thinks that their transition will eventually include a vaginoplasty, which constructs a vagina, a scrotectomy may not be recommended because the scrotal tissue could later be used to create the vaginal lining. [11]
Risks of Removing the Testicles
The risks of this surgery are typical of many surgical risks, which include bleeding or infection, injury to surrounding organs, scarring, or dissatisfaction with results. Other risks include nerve damage or loss of feeling, infertility, decreased libido (sex drive) and energy, and osteoporosis (a condition where bones become weak or brittle). [11]
However, the benefit of this procedure is that one’s body will produce less testosterone, which may may make it possible to reduce the dose of feminizing hormones. [11]
Penile Inversion Vaginoplasty
Before genital surgery (including removal of the testicles), surgeons who follow the WPATH standards of care usually require candidates for surgery to live at least for a year in their preferred gender role before the procedure (this is called the Real-Life Experience or the Real-Life Test). The goal of the Real-Life Test is to expose the individual to social issues that could arise if they were to continue to medically transition. By gradually changing their physical appearance, individuals will be able to observe how this change impacts various aspects of their life. Through the Real-Life Test, individuals may realize that they only want to socially transition. In other cases they may realize they want to continue down the medical transition path. By actively experiencing their new reality they are able to establish new behavior patterns, overcome social challenges, and make a more informed decision going forward. Furthermore, the Real-Life Test shows the surgeon that the individual is invested in the surgery and is committed to this irreversible procedure. [3, 26]
Penile inversion vaginoplasty is the surgical procedure that male to female transgender patients undergo to change their penis into a vagina. The testicles and most of the penis are removed and the urethra is cut shorter. Some of the skin is used to create a functional vagina, which is made out from the space between the urethra and rectum. [21] Then a “neoclitoris” (new clitoris) is constructed from the sensitive skin at the top of the penis. This is so arousal sensations can eventually be felt in the genital area. [3]
Plastic surgeons consider penile inversion vaginoplasty to be the gold standard genital reconstruction technique. [21] It is also recommended by the Center of Excellence for Transgender Health. [22]
Penile Inversion Vaginoplasty Risks
Surgical risks include bleeding, infection, rupture of the surgical sutures, and complete or partial cell death (necrosis) of the vagina and labia. Other risks include an abnormal connection (fistulas) from the bladder or bowel into the vagina, narrowing (stenosis) of the urethra, and vaginas that are either too short or too small for sex. While the surgical techniques for creating a vagina that looks good and functions correctly are impressive, some patients are unable to achieve orgasm. Furthermore, a second labiaplasty (plastic surgery that alters the labia minora and labia majora) may be needed to make visual adjustments. [1]
Healthline, a website that provides health and wellness information, recommends the following after penile inversion vaginoplasty surgery: [21]
· Don’t take a bath or submerge the body in water for eight weeks
· Don’t do strenuous activity for six weeks
· Don’t swim or ride a bike for three months
· Showering is fine after the first postoperative visit
· Do sit on a donut ring for comfort
· Don’t have sexual intercourse for three months
· Do apply ice for 20 minutes every hour of the first week
· Don’t worry about swelling
· Do expect vaginal discharge and bleeding for the first four to eight weeks
· Do avoid tobacco products for at least one month
· Be careful of pain medication; take it only as long as absolutely necessary
Bottom Line
Throughout the transgender transition process, each person should consider what is best for their social and medical needs. Since this is a serious medical and psychological process, it is essential that patients consult with a doctor that they trust. NEVER accept medical treatment from a non-licensed physician, and always choose a physician who is board certified in the relevant medical field. Patients should pay close attention to the laws and policies of their state and work with their insurance company to see what treatments will be covered.
There is not just one “right” way to transition. Each person should think about what is best for their mind and body. They should consider the risks and benefits of each option, and then decide which treatments are best for their transition process.
All articles are reviewed and approved by Dr. Diana Zuckerman and other senior staff.
The National Center for Health Research is a nonprofit, nonpartisan research, education and advocacy organization that analyzes and explains the latest medical research and speaks out on policies and programs. We do not accept funding from pharmaceutical companies or medical device manufacturers. Find out how you can support us here.
References
[1] World Professional Association for Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People. 2012. https://www.wpath.org/media/cms/Documents/SOC%20v7/Standards%20of%20Care_V7%20Full%20Book_English.pdf
[2] Planned Parenthood. What Are Appropriate Labels; Terms For Transgender People? PlannedParenthood.com. www.plannedparenthood.org/learn/sexual-orientation-gender/trans-and-gender-nonconforming-identities/transgender-identity-terms-and-labels.
[3] Bernstein, Lenny. Here’s How Sex Reassignment Surgery Works. The Washington Post, WP Company.www.washingtonpost.com/news/to-your-health/wp/2015/02/09/heres-how-sex-reassignment-surgery-works/. February 9, 2015.
[4] O’Keefe Osborn, Corinne. Your Guide to Anti-Androgens. Healthline.com. www.healthline.com/health/anti-androgen#types. February 5, 2018.
[5] Meyer, W. J. III. Webb, A., Stuart, C. A., Finkelstein, J. W., Lawrence, B., & Walker, P. A. Physical and hormonal evaluation of transsexual patients: A longitudinal study. Archives of Sexual Behavior. 1986.
[6] Breast Implant Information. Breast Implant Types. Breastimplantinfo.com. http://breastimplantinfo.org/breast-implant-types/.
[7] Breast Implant Information. Risks & Complications. Breastimplantinfo.com. http://breastimplantinfo.org/risks-complications/.
[8] Breast Implant Information. Making Your Decision. Breastimplantinfo.com. http://breastimplantinfo.org/making-your-decision/.
[9] Breast Implant Information. Types of Breast Implants. Breastimplantinfo.com. http://breastimplantinfo.org/types-breast-implants/. August 6, 2019.
[10] U.S. Food and Drug Administration, FDA. FDA Warns Against Use of Injectable Silicone for Enhancement. FDA.gov. https://www.fda.gov/medical-devices/safety-communications/fda-warns-against-use-injectable-silicone-body-contouring-and-enhancement-fda-safety-communication. November 14, 2017.
[11] Pai, Aditi. Healthline. What You Should Know About Orchiectomy for Transgender Women. Healthline.com. https://www.healthline.com/health/orchiectomy-for-transgender-women#orchiectomy-vs-scrotectomy. October 12, 2017.
[12] Hair Removal | Transgender Care. Hair Removal. Transcare.ucsf.edu. https://transcare.ucsf.edu/guidelines/hair-removal. June 17, 2016.
[13] Hession MT, Markova A, Graber EM. A review of hand-held, home-use cosmetic laser and light devices. Dermatol Surgery. https://www.ncbi.nlm.nih.gov/pubmed/25705949. March 2015.
[14] Gender Confirmation. Hair Removal Tips for MTF Transgender Patients. Genderconfirmation.com. https://www.genderconfirmation.com/hair-removal-options/.
[15] Ercolano, Alexa. FAQ: Facial Gender Surgery: The Johns Hopkins Center for Transgender Health. https://www.hopkinsmedicine.org/center-transgender-health/services-appointments/faq/facial-gender-surger. November 11, 2019.
[16] Spiegel, Jeffrey. The Spiegel Center. What Is a Trachea Shave Procedure? https://www.drspiegel.com/transgender/what-is-a-trachea-shave-procedure/. July, 19, 2013.
[17] Your Cosmetic Source. Tracheal Shave – Learn about This Delicate Transgender Surgery. Yourplasticsurgeryguide.com. https://www.yourplasticsurgeryguide.com/reconstructive/tracheal-shave/.
[18] Deschamps-Braly, Jordan, and Loren Schechter. American Society of Plastic Surgeons. Facial Feminization Surgery Risks and Safety. Plasticsurgery.org. https://www.plasticsurgery.org/reconstructive-procedures/facial-feminization-surgery/safety.
[19] Mayo Clinic, Mayo Foundation for Medical Education and Research. Facial Feminization Surgery. MayoClinic.com. https://www.mayoclinic.org/tests-procedures/facial-feminization-surgery/about/pac-20467962. September 11, 2019.
[20] Trans bodies, trans selves: a resource for the transgender community /edited by Laura Erickson-Schroth.New York: Oxford University Press, USA, 2014. Ch. 12 – Medical Transition – Maddie Deutsch.
[21] Healthline. Vaginoplasty: Gender Confirmation Surgery. Healthline.com. https://www.healthline.com/health/transgender/vaginoplasty#technique.
[22] Vaginoplasty Procedures, Complications and Aftercare | Transgender Care. Vaginoplasty Procedures, Complications and Aftercare. https://transcare.ucsf.edu/guidelines/vaginoplasty. June 17, 2016.
[23] American Psychiatric Association. What Is Gender Dysphoria? Psychiatry.org. https://www.psychiatry.org/patients-families/gender-dysphoria/what-is-gender-dysphoria. February, 2016.
[24] American Heart Association. ScienceDaily. Hormone therapy may increase cardiovascular risk during gender transition. Sciencedaily.com.
[25] Helpline. Laser Hair Removal vs. Electrolysis: Which Is Better? Helpline.com. https://www.healthline.com/health/beauty-skin-care/laser-hair-removal-vs-electrolysis#laser-hair-removal
[26] TransHealth. Origins of the Real-Life Test. Trans-health.com. http://www.trans-health.com/2003/real-life-test/. January 20, 2003.
Samantha Newman, National Center for Health Research
The focus of this article is medical transitioning from female to male, the process by which transgender individuals change the way they look so that their physical characteristics match the gender they feel. [2] Transgender is defined as individuals whose social or psychological gender identity is different than their sex assigned at birth. [2]
Transitioning isn’t necessarily medical. It can involve changing one’s name or one’s pronouns (such as changing she/her/hers to he/him/his and vice versa). It can involve changing the way one dresses. Medical transitioning can involve medical treatments, such as taking hormones or getting surgery. Experts agree that there is not one “right” way to transition. Transitioning can involve any combination of these changes or it can be any change that allows someone to more comfortably present to the world. [2] What is most important is that someone’s transition process reflects their needs and what works best for them and their body. [1] While there are many social ways to transition, such as coming out to friends, using different pronouns, or using a different name, this article will specifically examine the medical treatment options in the female to male transition process. (Our article on medical transitioning from male to female is available here.)
For someone considering medical transitioning, it is important to know the risks that are associated with specific medical treatments and to decide if the likely benefits outweigh those risks. It is essential to realize that many aspects of this medical transition can be very expensive, so make sure to find out what will or will not be covered by insurance. The goal of this article is to provide information to help individuals make an informed choice, choosing the safest options that will provide the most benefit.
Before beginning transgender transitional medical treatment, the World Professional Association for Transgender Health (WPATH) recommends meeting with a mental health professional for a gender dysphoria diagnosis and psychotherapy. [1] According to the American Psychiatric Association, a gender dysphoria diagnosis is when a person’s physical or assigned gender (such as someone born female or born male) does not match the gender they feel (for example, feeling they are male or female). [23] Most doctors will not offer most medical transitioning options unless the individual has this diagnosis. Some medical procedures do not require meeting with a mental health professional beforehand, but having a supportive mental health professional can be helpful in this process.
After receiving a gender dysphoria diagnosis, deciding whether or not to choose hormone therapy is often the first step. If a person chooses hormone therapy, it is usually followed by a period of living publicly as a trans man (biologically female who identifies as male) or trans woman (biologically male who identifies as female) before major surgeries are performed. This is called the Real-Life Test and it will be discussed later in the article. [3] Hormone therapy is usually recommended prior to most types of trans surgery. [1]
Each medical intervention has its own unique benefits and risks.
For trans men, medical transitioning may include any of the following:
- Hormone therapy (to create masculine characteristics such as a deeper voice, facial hair growth, redistribution of body fat away from hips and breasts, and not getting a period.
- Male chest reconstruction, or “top surgery” (to remove the breasts and breast tissue)
- Hysterectomy and salpingo-oophorectomy (to remove female reproductive organs such as the uterus and ovaries/fallopian tubes)
- Phalloplasty or “bottom surgery” (construction of a penis using skin from other parts of the body). [2] Metoidioplasty is a type of “bottom surgery” that causes the clitoris to work more like a penis, which is accompanied by hormone treatment to make the clitoris grow larger [2]
Hormone Therapy
There are many types of hormones in our bodies, but estrogen, testosterone, and progestogen are considered sex hormones because they affect characteristics that influence aspects of the body as well as sexual desire. All males and females have estrogen, testosterone, and progestogen, but the relative amounts of these hormones in the body give us our specific physical characteristics. [20] In female to male trans patients, testosterone is taken to help develop male characteristics. [1] The characteristics that could develop include a deeper voice, growth of the clitoris, growth in facial and body hair, the stopping of one’s menstrual cycle, decrease in breast tissue, increase in sex drive, and more muscle mass than body fat. [1]
According to WPATH, the criteria for hormone therapy are as follows:
1. Persistent, well-documented gender dysphoria diagnosis by a qualified mental health professional;
2. Capacity to make a fully informed decision and to consent for treatment;
3. Age of majority (which varies in different countries and states). If a person wanting to transition is younger, there are different rules that can be found in Section VI of the WPATH’s Standard of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People);
4. If an individual who wants to transition already has significant medical or mental health issues, those mental health issues must be reasonably well controlled. [1]
Most physical changes occur gradually over the course of two years. The amount of physical change and the exact timeline of those changes vary. For more details, see Table 1, which outlines the effects and expected time these effects will take place once hormones are taken as presented in WPATH’s Standard of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People. [1]
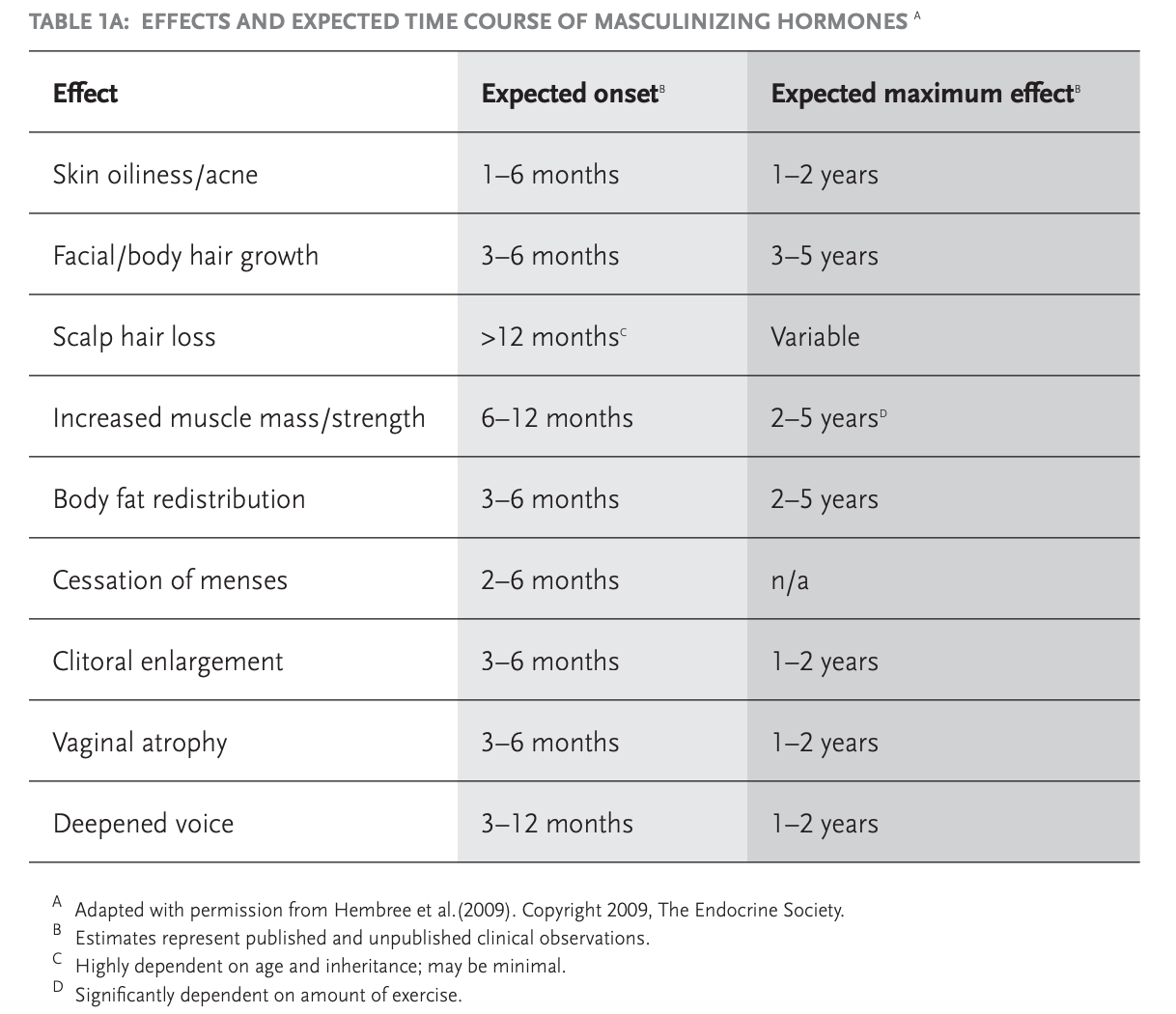
Table 1 taken from WPATH’s Standard of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People
Testosterone can be administered in various forms, but the most popular are hormone injections. Some choose to begin on a lower dose and increase slowly, while others chose to begin at a standard dose. It’s important to discuss these options with your doctor. [3]
Risks of Hormone Therapy
All medical treatments have risks. According to WPATH, masculinizing hormone therapy can cause a likely increased risk of higher red blood cell count in the body (polycythemia), weight gain, acne, balding, and sleep apnea. [1] Other possible risks include elevated liver enzymes, an increase in fats or lipids in the blood (hyperlipidemia), worsening of an underlying psychotic condition, cardiovascular disease and heart attacks, abnormally high blood pressure (hypertension), and Type 2 diabetes. [1] It has not been proven whether or not masculinizing hormone therapy increases the risk of breast cancer, cervical cancer, ovarian cancer, or uterine cancer if those organs are not removed. [1]
The effects of hormone therapy are seen gradually over a period of about two years. It is important to understand that taking higher than prescribed doses of hormones DOES NOT increase the speed of the transition process. [1] It can, however, cause dangerous side effects. [4] For example, excess testosterone can be converted to estrogen, which may increase the risks of uterine imbalance or cancer. However, as mentioned above, taking a prescribed amount of testosterone by a physician has not proven to increase the risk of cancer. [3]
Most importantly, never take hormones from overseas mail-order companies, street sellers, neighbors, or friends. Always go to a licensed physician because they will be able to administer the best dosage of these hormones as well as properly monitor their effects. [4]
Oral testosterone or synthetic male sex hormone (androgen) medication shouldn’t be used because of potential adverse effects on your liver and lipids. [5] Read more about hormone therapy at Masculinizing Hormone Therapy.
Because masculinizing hormone therapy might reduce the fertility a trans individual had as a woman, it’s important to make decisions about freezing one’s eggs or other options before starting hormone therapy. [5] However, a trans man can still be at risk of pregnancy if the uterus and ovaries have not been removed. If one wants to avoid becoming pregnant, use a barrier form of contraception or an intrauterine device (IUD). [5]
Top Surgery
Male chest reconstructionTop surgery
The criteria for a mastectomy and the creation of a male chest in female-to-male patients is as follows:
1. Persistent, well-documented gender dysphoria by a qualified mental health professional;
2. Capacity to make a fully informed decision and to consent for treatment;
3. Age of majority in a given country;
4. If significant medical or mental health concerns are present, they must be reasonably well
controlled.
Hormone therapy is not a prerequisite for top surgery. [1]
Risks of Top Surgery
Similar to any other type of major surgery, top surgery for transgender men poses a risk of bleeding, infection, and an adverse reaction to anesthesia.
Other complications might include:
- Poor wound healing
- Fluid accumulation beneath the skin (seroma)
- A solid swelling of clotted blood within your tissues (hematoma)
- Damaged or dead body tissue (tissue necrosis), such as in the nipple
- Scarring
- Dissatisfaction with appearance after surgery
- Asymmetry [6]
After surgery, the chest should remain in a compression wrap for several weeks. There will likely be one or two small plastic tubes placed in the chest to drain any fluids that accumulate after surgery. [6] The surgeon will also recommend sleeping with the torso elevated for the first week after surgery. Avoid lifting more than 10 to 15 pounds for several weeks. [6]
Removal of the Uterus (hysterectomy) and Fallopian Tubes/Ovaries (salpingo-oophorectomy)
A hysterectomy is when a surgeon removes the uterus. A hysterectomy for transgender male patients is usually accompanied by a salpingectomy (removal of fallopian tubes) and a oophorectomy (removal of the ovaries). [1] Hysterectomy often includes removal of the cervix as well as the uterus. When the surgeon also removes the ovaries and fallopian tubes, it’s called a total hysterectomy with salpingo-oophorectomy. [11] However, a patient may make the choice to not remove the fallopian tubes and ovaries during a hysterectomy procedure.
The “best practice” for these surgical procedures in transgender patients has not been established. Hysterectomy may be performed abdominally, laparoscopically, or vaginally. An abdominal hysterectomy removes the uterus through an incision in the lower abdomen. [10] A vaginal hysterectomy removes the uterus through the vagina. [11] A laparoscopic hysterectomy is a minimally invasive surgery; the surgeon makes a small incision in the belly button or in the vagina and inserts a tiny camera. [12]
For all types of patients, not just for transgender men, the vaginal approach has the fewest complications and blood loss, quickest recovery, and is considered the most cost-effective. [11] For transgender men, vaginal hysterectomy has the added benefit of leaving no abdominal scars. Studies also show that laparoscopic hysterectomy can successfully be accomplished without additional complications. [9]
The salpingo-oophorectomy surgery is located in the same region as a hysterectomy surgery, therefore making a total hysterectomy with salpingo-oophorectomy procedure a popular option for transgender patients. [14] There are three different types of salpingo-oophorectomy procedures. You can read about them here: https://www.healthline.com/health/salpingo-oophorectomy#procedure
Retaining or removing the ovaries and fallopian tubes at the time of a hysterectomy surgery is a personal decision based on the patient’s desires and future fertility plans. [9]
According to WPATH, the criteria for hysterectomy and salpingo-oophorectomy in trangender male patients is as follows:
1. Persistent, well-documented gender dysphoria;
2. Capacity to make a fully informed decision and to consent for treatment;
3. Age of majority in a given country;
4. If significant medical or mental health concerns are present, they must be well controlled.
5. 12 continuous months of hormone therapy as appropriate to the patient’s gender goals (unless
hormones are not clinically indicated for the individual). The aim of hormone therapy prior to genital surgery is primarily to introduce a period of reversible testosterone suppression, before the patient undergoes surgery that can’t be reversed. [1]
WPATH advises that “Two referrals—from qualified mental health professionals who have independently assessed the patient—are needed for genital surgery (i.e., hysterectomy/salpingo-oophorectomy, orchiectomy, genital reconstructive surgeries).” One of the referrals can be from the patient’s psychotherapist. [1]
Before genital surgery (hysterectomy, salpingo-oophorectomy, phalloplasty, or metoidioplasty surgery), surgeons who follow the WPATH standards of care usually require candidates for surgery to live for at least a year in their preferred gender role before the procedure. [1] This is called the Real-Life Experience or the Real-Life Test, and the goal is to expose the individual to social issues that could arise if they were to continue to medically transition. By gradually changing their physical appearance, individuals will be able to observe how this change affects various aspects of their life. Through the Real-Life Test, individuals may realize that they only want to socially transition or they may realize they want to continue down the medical transition path. [7,8] By actively experiencing their new reality they are able to overcome social challenges and make a more informed decision going forward. In addition, the Real-Life Test shows the surgeon that the individual is committed to this irreversible procedure. [7, 8]
Risks of Hysterectomy
The risk of a hysterectomy depends on the type of procedure performed. A hysterectomy is generally very safe. However, there are risks with any major surgery, as noted earlier in this article. Risks associated specifically with a hysterectomy include blood clots; infection; excessive bleeding; damage to the urinary tract, bladder, rectum or other pelvic structures during surgery; or earlier onset of menopause even if the ovaries aren’t removed. [10] Rarely, complications can be fatal [10]
There also might be scarring, but it depends on the type of incision made during the abdominal hysterectomy. [10] As a whole this type of procedure has generally been shown to be less desirable to transgender patients due to visible scarring, longer hospital time, and longer recovery time.
Vaginal hysterectomy involves a shorter time in the hospital, lower cost and faster recovery than an abdominal hysterectomy. [11]
In addition to the risks above, there are specific risks associated with a laparoscopic hysterectomy:
- It can take longer to perform compared with abdominal or vaginal surgery
- There is an increased risk of injury to the urinary tract and other organs
Following surgery, one can expect to have some pain for the first few days. Pain medication is usually prescribed. There will be bleeding and discharge from the genital area for several weeks. Sanitary pads can be used after the surgery. [13]
Risks of Fallopian Tubes/Ovaries (salpingo-oophorectomy) Removal Surgery
Salpingo-oophorectomy is considered a relatively safe procedure, but as with any surgery, it has risks. These mostly include bleeding, blood clots, infection, or a bad reaction to anesthesia.
Other risks of the removal of the Fallopian Tubes/Ovaries could include:
- Nerve damage
- Hernia
- Formation of scar tissue
- Bowel obstruction [14]
It is essential to call a doctor if there is redness or swelling at the incision site, fever, drainage or opening of the wound, increasing abdominal pain, excessive bleeding, foul-smelling discharge, difficulty urinating, nausea or vomiting, shortness of breath, chest pain, or fainting. [14]
A hysterectomy/salpingo-oophorectomy surgery can be combined with a metoidioplasty or phalloplasty, vaginectomy (removal of the vagina), scrotoplasty (construction of a scrotum), or implantation of erection and/or testicular prostheses. It’s important to talk to a physician about the risks and benefits of combining surgeries. [1]
Phalloplasty or Metoidioplasty Surgery aka “Bottom Surgery”
A phalloplasty constructs a penis. The goal is to build a cosmetically appealing penis that is capable of feeling sensations and releasing urine from a standing position. [15, 16]
According to WPATH, criteria for phalloplasty in transgender male patients:
1. Persistent, well-documented gender dysphoria by a qualified mental health professional;
2. Capacity to make a fully informed decision and to consent for treatment;
3. Age of majority in a given country;
4. If significant medical or mental health concerns are present, they must be well controlled;
5. 12 continuous months of hormone therapy as appropriate to the patient’s gender goals;
Although not required, it is recommended that these patients also have regular visits with a mental health or other medical professional. [1]
The current gold standard of phalloplasty surgery is known as a radial forearm free-flap (RFFF) phalloplasty. For this procedure, surgeons use a flap of skin from the forearm to build the shaft of the penis. [15] The clitoris is usually left in place near the base of the penis, where it can still be stimulated. [15]
The RFFF procedure provides penile skin sensitivity as well as good aesthetic results. The urethra can also easily be constructed in a tube-within-a-tube fashion. This is important to allow for standing urination. [15]
Metoidioplasty, also known as a meta, is a surgical procedure that uses the patient’s existing genital tissues to form a new penis. [19] It can be performed by growing the clitorius with testosterone. Doctors tend to recommend being on testosterone therapy at least one to two years before this procedure. [19]
Pros and Cons of Metoidioplasty compared to a Phalloplasty procedure
Pros
- Fully functioning penis (can become erect on its own)
- Minimal visible scarring
- Fewer surgical procedures than phalloplasty
- Can also have a phalloplasty later if one chooses
- Shorter recovery time
- Significantly less expensive than phalloplasty, if not covered by insurance: ranges from $2,000 to $20,000 versus $50,000 to $150,000 for phalloplasty [19]
Cons
- New penis relatively small in length and girth (measuring anywhere from 3 to 8 cm in length)
- Penetration during sex may not be possible
- Requires use of hormone replacement therapy and substantial clitoral growth
- May not be able to urinate while standing [19]
Risks of Metoidioplasty Surgery
As mentioned about, with any surgery there is a risk of infection, bleeding, blood clots, damage to surrounding tissues, pain, negative reactions to anesthesia or other medications. However, metoidioplasty has some unique risks as well. [18]
Risks associated with metoidioplasty surgery include:
- Urethral complications, the most common one is a urinary fistula, which is an opening in the urethra that causes urine leakage
- Wound breakdown (ruptures along the incision lines)
- Bladder or rectal injury
- Dissatisfaction with the size or shape of the penis
- Inability to stand-to-pee [18]
Some long term complications can include scarring or urethral issues that cause difficulty or prevent urine from going through. [18]
You can learn about different types of metoidioplasty procedures by visiting this website: https://www.healthline.com/health/transgender/metoidioplasty
Bottom Line
Throughout the transgender transition process, each person should consider what is best for their social and medical needs. Since this is a serious medical and psychological process, it is essential that patients consult with a doctor that they trust. NEVER accept medical treatment from a non-licensed physician, and always choose a physician who is board certified in the relevant medical field. Patients should pay close attention to the laws and policies of their state and work with their insurance company to see what treatments will be covered.
There is not just one “right” way to transition. Each person should think about what is best for their mind and body. They should consider the risks and benefits of each option, and then decide which treatments are best for their transition process.
All articles are reviewed and approved by Dr. Diana Zuckerman and other senior staff.
The National Center for Health Research is a nonprofit, nonpartisan research, education and advocacy organization that analyzes and explains the latest medical research and speaks out on policies and programs. We do not accept funding from pharmaceutical companies or medical device manufacturers. Find out how you can support us here.
References
[1] World Professional Association for Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People. 2012. https://www.wpath.org/media/cms/Documents/SOC%20v7/Standards%20of%20Care_V7%20Full%20Book_English.pdf
[2] Planned Parenthood. What Are Appropriate Labels; Terms For Transgender People? PlannedParenthood.com. www.plannedparenthood.org/learn/sexual-orientation-gender/trans-and-gender-nonconforming-identities/transgender-identity-terms-and-labels.
[3]. Deutsch, Maddie. Transcare UCSF. Information on Testosterone Hormone Therapy. Transcare.ucsf. https://transcare.ucsf.edu/article/information-testosterone-hormone-therapy.
[4] Trans bodies, trans selves: a resource for the transgender community /edited by Laura Erickson-Schroth.New York: Oxford University Press, USA, 2014. Ch. 12 – Medical Transition. Dr. Maddie Deutsch.
[5] Mayo Clinic, Mayo Foundation for Medical Education and Research. Masculinizing Hormone Therapy. Mayoclinic.org. April 14, 2020. https://www.mayoclinic.org/tests-procedures/ftm-hormone-therapy/about/pac-20385099
[6] Mayo Clinic, Mayo Foundation for Medical Education and Research. Top Surgery for Transgender Men. Mayoclinic.org. September 27, 2019, https://www.mayoclinic.org/tests-procedures/top-surgery-for-transgender-men/about/pac-20469462
[7] Bernstein, Lenny. Here’s How Sex Reassignment Surgery Works. The Washington Post, WP Company.www.washingtonpost.com/news/to-your-health/wp/2015/02/09/heres-how-sex-reassignment-surgery-works/. February 9, 2015.
[8] TransHealth. Origins of the Real-Life Test. Trans-health.com. http://www.trans-health.com/2003/real-life-test/. January 20, 2003.
[9] Obedin-Maliver, Juno. Transcare UCSF. Hysterectomy. Transcare.ucsf. June 17, 2016. https://transcare.ucsf.edu/guidelines/hysterectomy
[10] Mayo Clinic, Mayo Foundation for Medical Education and Research. Abdominal Hysterectomy. Mayoclinic.org. July 25, 2019. https://www.mayoclinic.org/tests-procedures/abdominal-hysterectomy/about/pac-20384559
[11] Mayo Clinic, Mayo Foundation for Medical Education and Research. Vaginal Hysterectomy. Mayoclinic.org. Feb. 8, 2020. https://www.mayoclinic.org/tests-procedures/vaginal-hysterectomy/about/pac-20384541
[12] McMacken, Melissa. Johns Hopkins Medicine. Laparoscopic Hysterectomy. Hopkinsmedicine.org. Feb. 2, 2018. https://www.hopkinsmedicine.org/gynecology_obstetrics/specialty_areas/gynecological_services/treatments_services/minimally_invasive_gynecologic_robotic_surgery/treatments/laparoscopic_hysterectomy.html
[13] ACOG. Hysterectomy Frequently Asked Questions: Special Procedure. Acog.org. https://www.acog.org/Patients/FAQs/Hysterectomy?IsMobileSet=false#hysterectomy
[14] Pietrangelo, Ann. What to Expect from Salpingo-Oophorectomy. Healthline. Healthline.com. Feb. 13, 2001. https://www.healthline.com/health/salpingo-oophorectomy#procedure
[15] Osborn, Corinne O’Keefe. Phalloplasty: FTM Gender Confirmation Surgery Recovery, Complications. Healthline. Healthline.com. May 7, 1983. https://www.healthline.com/health/transgender/phalloplasty
[16] Ercolano, Alexa. FAQ: Phalloplasty: The Johns Hopkins Center for Transgender Health. The Johns Hopkins Center for Transgender Health. Hopkinsmedicine.org. Sept. 17, 2019. https://www.hopkinsmedicine.org/center-transgender-health/services-appointments/faq/phalloplasty
[17] Boston Children’s Hospital. Metoidioplasty: Boston Children’s Hospital. Childrenshospital.org. http://www.childrenshospital.org/conditions-and-treatments/treatments/metoidioplasty
[18] Trans Media Network. Metoidioplasty Risks and Complications: Is Metoidioplasty Really Worth It?. Metoidioplasty.net. https://www.metoidioplasty.net/risks-complications/
[19] Clements, KC. Metoidioplasty: Surgery, Results, and Recovery. Healthline. Healthline.com May 7, 1983. https://www.healthline.com/health/transgender/metoidioplasty





































